What Is a Stable Surgical Guide? A Complete Introduction for Dental Professionals
Implant dentistry has evolved significantly over the past two decades. What was once a freehand procedure relying almost entirely on the surgeon’s tactile skill. Spatial judgment is now a digitally planned, precisely guided workflow, and at the center of that transformation is the surgical guide.
But not all surgical guides are equal. Among the variables that determine whether a guided implant surgery succeeds or fails, stability stands out as the most fundamental. A guide that moves, flexes, or sits inaccurately introduces errors that no amount of surgical skill can fully correct.
This article provides a complete clinical introduction to stable surgical guides.
What Is a Stable Surgical Guide?
Basic Definition of a Surgical Guide in Implant Dentistry
A surgical guide, also called a surgical template, drill guide, or implant stent, is a custom-fabricated device used during dental implant placement to transfer a virtually planned implant position from a digital treatment plan into the patient’s mouth with precision.
In its most fundamental form, a surgical guide is a rigid or semi-rigid appliance that seats over the patient’s existing anatomy and contains one or more metal sleeves or guiding channels. These channels direct the surgical drill along a specific axis, at a specific angulation, and to a specific depth. It is exactly as planned in the preoperative software.
Cone Beam Computed Tomography (CBCT)
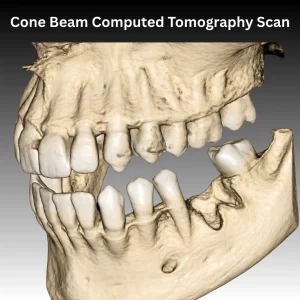 The process begins with a Cone Beam Computed Tomography (CBCT) scan, which provides a three-dimensional image of the patient’s bone volume, anatomy, and critical structures. This CBCT data is merged with an intraoral scan or digital impression of the dentition and soft tissue.
The process begins with a Cone Beam Computed Tomography (CBCT) scan, which provides a three-dimensional image of the patient’s bone volume, anatomy, and critical structures. This CBCT data is merged with an intraoral scan or digital impression of the dentition and soft tissue.
Using implant planning software, the clinician virtually positions the implant in the ideal prosthetically driven location. Account for bone density, available volume, proximity to the inferior alveolar nerve or sinus floor, and the planned final restoration.
Approval of Virtual Plan:
Once the virtual plan is approved, the surgical guide is designed digitally and fabricated, either through 3D printing or CAD/CAM milling, as a precise physical representation of that plan. When seated correctly in the patient’s mouth, it restricts drill movement to the planned trajectory, preventing the deviations in angulation, depth, and position that freehand placement is susceptible to.
The result, when done correctly, is implant placement that closely matches the virtual plan, which is predictable, reproducible, and prosthetically driven from the outset.
What Makes a Surgical Guide “Stable” vs Unstable?
Stability is not optional. This is the minimum requirement for a guide to function as intended. Even a one-degree deviation in drill angulation can produce meaningful displacement at the implant apex level. Particularly in longer implants or when proximity to anatomical structures is a concern.
A stable surgical guide does three things:
- Sets firmly on the patient’s anatomy, with no rocking, tilting, or gaps
- Stays immobile during drilling, no shifting or flexing under pressure
- Resets to exactly the same position every time it is removed and replaced
An unstable guide fails on one or more of these. It may rock on the soft tissue, tilt at a free-end extension, or flex during osteotomy preparation. Even a one-degree deviation in drill angulation produces measurable displacement at the implant apex level. enough to compromise the prosthetic outcome or endanger adjacent structures.
How Do Stable Surgical Guides Differ from Conventional Guides?
Before the era of digital planning and computer-aided implant surgery, surgical templates were considerably simpler. Conventional guides are typically fabricated from a diagnostic wax-up or a duplicate of a removable prosthesis, with drilled channels indicating approximate implant locations. They provided directional guidance but not precision control.
These conventional guides lacked several properties that define a modern, stable surgical guide:
- No CBCT integration: Conventional guides were not based on three-dimensional bone data. These models can indicate where a tooth should emerge but cannot account for the actual bone volume, angulation constraints, or proximity to nerves and sinuses beneath the surface.
- No drill depth control: Conventional templates often guided the initial drill direction but provided no mechanism for controlling how deep the osteotomy was prepared.
- Variable stability: Conventional guides were not always designed with retention and stability as primary engineering considerations. Fit was often approximate.
- No sleeve system: Without metal sleeves to guide the drill, even a well-seated conventional guide introduces angular error through lateral drill movement within the channel.
Modern Stackable Surgical Guides address all of these limitations. They are designed from merged CBCT and intraoral scan data, fabricated with precision manufacturing, incorporate metal sleeves that constrain drill movement, and are engineered with specific support and retention mechanisms appropriate to the patient’s anatomy.
Why Does Stability Matter in a Surgical Guide?
How Does Guided Stability Work? Directly Affect Implant Accuracy?
Implant accuracy is measured by comparing the planned position with the actual postoperative position. It was assessed by superimposing the preoperative plan on the postoperative CBCT scan.
Deviations are recorded at three points:
- The implant collar
- The apex
- The angular axis
Guide stability is one of the strongest predictors of these measurements. A 2026 study in the Journal of Functional Biomaterials evaluated 180 implants across three support types and confirmed guide support as a statistically significant factor in surgical accuracy (p < 0.001).
- Tooth-supported guides consistently produced the lowest deviations.
- Mucosa- and bone-supported guides showed greater variability, especially at the apex, where instability errors are most amplified.
Any guide movement during drilling transfers directly to the drill. A 0.5mm lateral shift during a 10mm osteotomy produces greater error at the apex than at the collar. A guide that tilts under pressure creates angular deviation that grows with depth.
A stable, fully seated guide eliminates these variables entirely.
Risks of Using an Unstable Surgical Guide
The risks associated with unstable surgical guides span the clinical, biological, and prosthetic domains. Every dental professional using guided implant surgery should understand them clearly.
Anatomical Risk: Damage to Critical Structures
An implant placed off-axis due to guide instability can encroach on the inferior alveolar nerve, perforate the sinus floor, impinge on adjacent tooth roots, or breach the cortical plate. These are serious complications that may require immediate intervention and can result in permanent neurosensory disturbance, implant failure, or loss of adjacent teeth.
Prosthetic Risk: Misalignment with the Planned Restoration
Implants are placed with a specific emergence profile and angulation required by the planned crown, bridge, or overdenture. A deviated implant may emerge at an angle or position incompatible with the restoration, forcing the clinician to use angled abutments, accept compromised aesthetics, or, in severe cases, remove and replace the implant.
Biological risk: Compromised Osseointegration
An implant placed in the wrong position within the bone may be inadequately supported by cortical or trabecular structure, resulting in insufficient primary stability. Without adequate primary mechanical stability at placement, the conditions for successful osseointegration are compromised, increasing the risk of early implant failure.
Clinical Risk: The Need for Unplanned Intervention
Complications arising from inaccurate placement may require additional procedures: grafting, nerve decompression, implant removal, or restorative revision. All of which increase patient risk, extend treatment time, and carry high cost and liability implications.
How Does Stability Lead to Predictable Clinical Outcomes?
When a guide is seated accurately and stays immobile throughout surgery, outcomes become predictable. This predictability is one of the most valuable things a dental professional can offer.
Predictable placement means the clinician knows before surgery exactly where the implant will be, at what angulation, and how the restoration will connect. Abutments and provisionals can be fabricated ahead of the surgery date and delivered immediately. The entire prosthetic workflow is compressed.
For patients, shorter procedures, less discomfort, and confidence that the result matches what was planned. For the practice, less chair time, fewer remakes, and a stronger clinical reputation.
A stable guide is what turns a digital plan into a clinical reality.
Conclusion
As digital workflows continue to evolve, clinicians increasingly rely on experienced laboratory partners capable of designing and manufacturing highly precise, stable surgical guides tailored to individual clinical requirements. At Confident Dental Lab, we understand that stability is not simply a feature; it is the foundation of successful guided surgery. Through advanced digital planning, precision manufacturing, and close collaboration with dental professionals, we help deliver surgical guides designed for accuracy, consistency, and predictable implant outcomes.
Latest News

Full Arch Guided Implant Surgery: Choosing the Right Surgical Guide
A stable surgical guide is a key factor in successful implant dentistry, ensuring precise transfer of digital plans into the patient’s mouth. Excellence in 2026.
Stackable Surgical Guides in Dentistry: The Future of Precise Dental Implants Surgery
Advances in intraoral scanning, optimized scan protocols, and lab-driven validation provide clinicians and dental labs with powerful tools for excellence in 2025.

ICAM Photogrammetry: How Confident Dental Lab Delivers Once‑Impossible Full‑Arch Implant Precision
Advances in intraoral scanning, optimized scan protocols, and lab-driven validation provide clinicians and dental labs with powerful tools for excellence in 2025.
Zirconia Crowns: Benefits, Types, and Why Dentists Prefer Them
Zirconia crowns consist of zirconium dioxide, a crystalline ceramic engineered for exceptional toughness in restorative dentistry.